Persistent left atrial tachycardia after atrial fibrillation ablation – Successful catheter ablation
Clinical history: This 61-year-old man presented with sustain atrial tachycardia lasting for at least 6 months. The patient has a history of surgically repaired mitral valve 13 years before, and 2 ablation procedures (2010 and 2012) for persistent atrial fibrillation comprised circumferential pulmonary vein isolation.
ECG (on admission): atrial tachycardia with 1:1 conduction 187bpm with positive P wave in V1-V2 and isoelectric the inferior leads (Fig. a)
EP Study –Ablation:
Procedure: After informed consent was obtained, the patient was brought to the electrophysiology lab where ECG and vital signs were continuously monitored. The right and left groin was meticulously prepared with Betadine solution and was draped in the usual sterile fashion. Lidocaine 1% was administered subcutaneously for local anesthetic. Using modified Seldinger technique, 4 introducer sheaths were inserted into the right and left femoral veins
EP catheters:
- A quadripolar fixed curve catheter inserted through the left femoral vein and positioned for His bundle recording and for right ventricular stimulation.
- A 10polar deflectable catheter inserted through the left femoral vein into the coronary sinus (CS).
- 20polar circular catheters for Pulmonary Vein (PV) mapping
- An irrigated 4 mm tip quadripolar deflectable mapping-ablation catheter
The system Ensite Velocity (St Jude Medical) was used for the three-dimensional mapping of the left atrium and the EP WorkMate Recording System (St. Jude Medical) for conventional mapping. (Fig. A). Thereafter, a double transseptal puncture was carried out in order to insert to the left atrium the circular PV mapping catheter and the ablation catheter. With the use of the ablation catheter a 3-D reconstructed model of the left atrium and the pulmonary veins was performed.
The initial recording sowed an atrial tachycardia with circle length 360ms, prematurity in His catheter and bracketing in CS poles (Fig. 1). The 20-pole circular catheter was placed sequentially into all the PVs confirming the isolation by sowing absence of PV potentials (Fig 2-5). With sequential mapping during AT a local activation time map (LAT map) was constructed sowing a centrifugal propagation pattern from the base of LAA (Fig. B, Video 1). The entrainment mapping was almost positive from the septal site of the LAA base (Fig. 5), and negative from LA roof and from CS (Fig. 6,7).
Ablation was applied in that area resulting in cycle length increase (from 360 to 400ms) (Fig. 8,9). The continuation of the lesion set terminated the tachycardia (Fig. 10). With high rate stimulation the tachycardia was re-induced (Fig. 11). More applications in the area stopped the tachycardia once again (Fig. 12). Then an anterior line was performed and confirmed by pacing maneuvers (Fig. C, Fig. 13). Another induction attempt, performed from CS, induced a tachycardia restricted in LAA area with exit block to the rest atrial myocardium (Fig. D, Video 2, Fig. 14,15). Thereafter, the circular catheter was placed into the LAA. The activation mapping guided the ablation of the premature point (Fig. 16), which finally eliminated the tachycardia (Fig 17). All the re-induction attempts with high rate atrial pacing failed to induce any tachycardia (Fig 18,19).
Post-operative course: The operation and post-operative course was uncomplicated. The patient was immediately anticoagulated with low molecular weight heparin and rivaroxaban. The patient is at sinus rhythm after 2 years of follow-up.
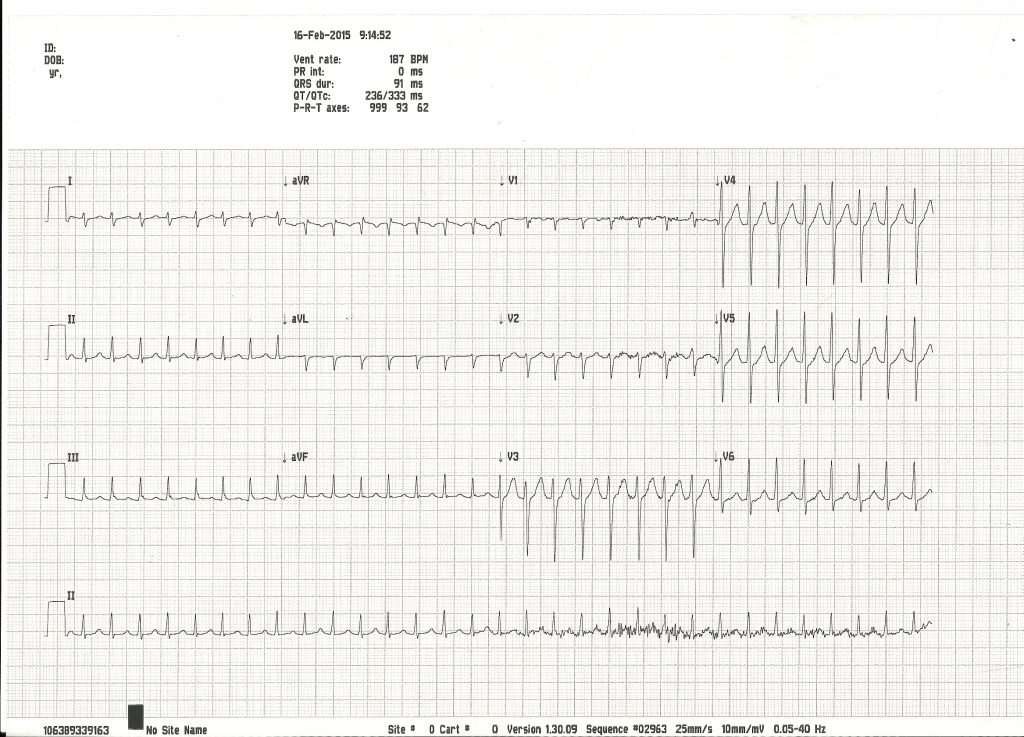
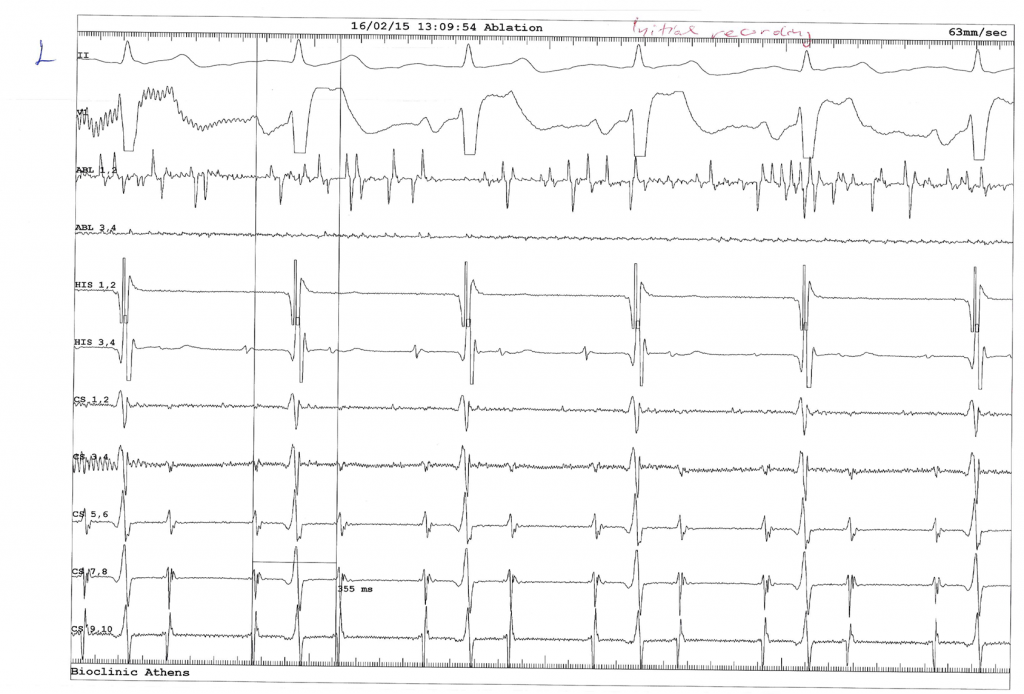
Fig. 1
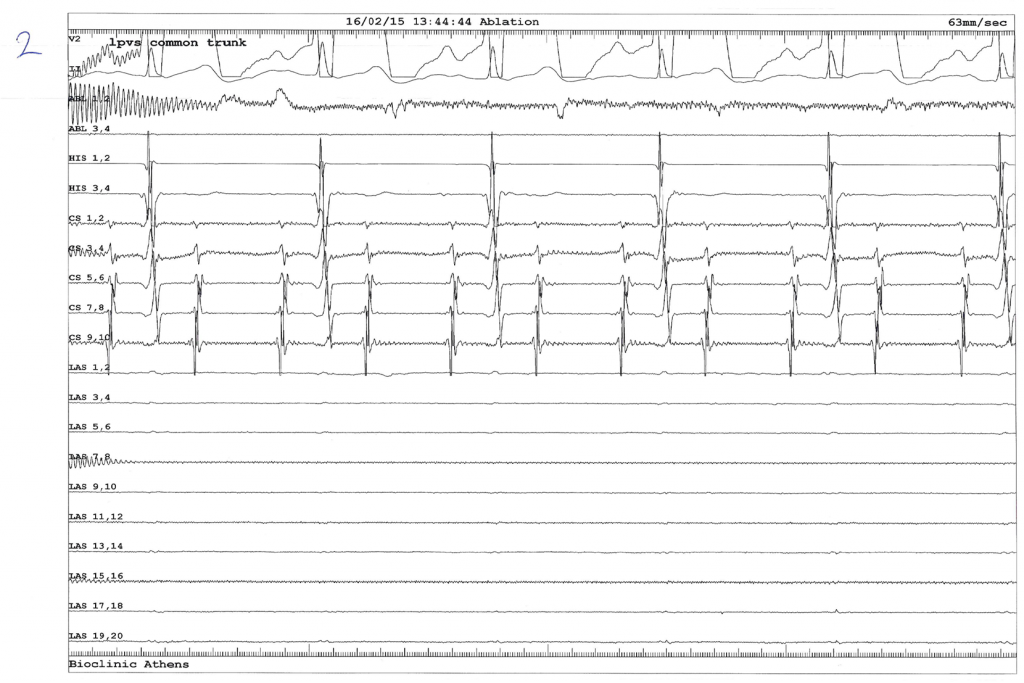
Fig. 2
Fig. 3
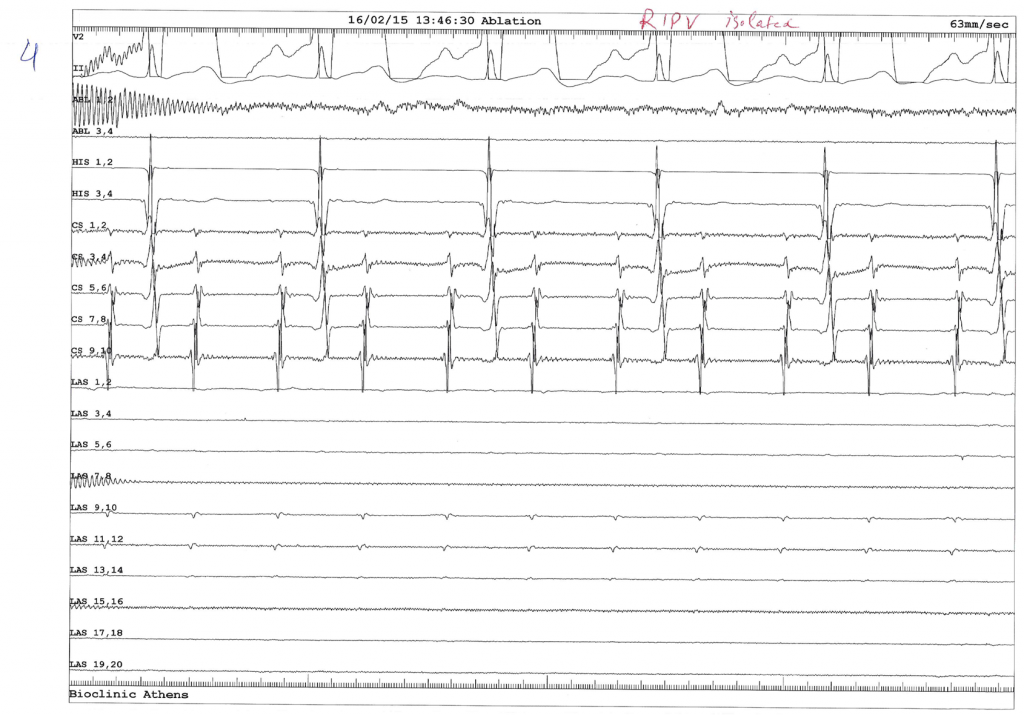
Fig. 4
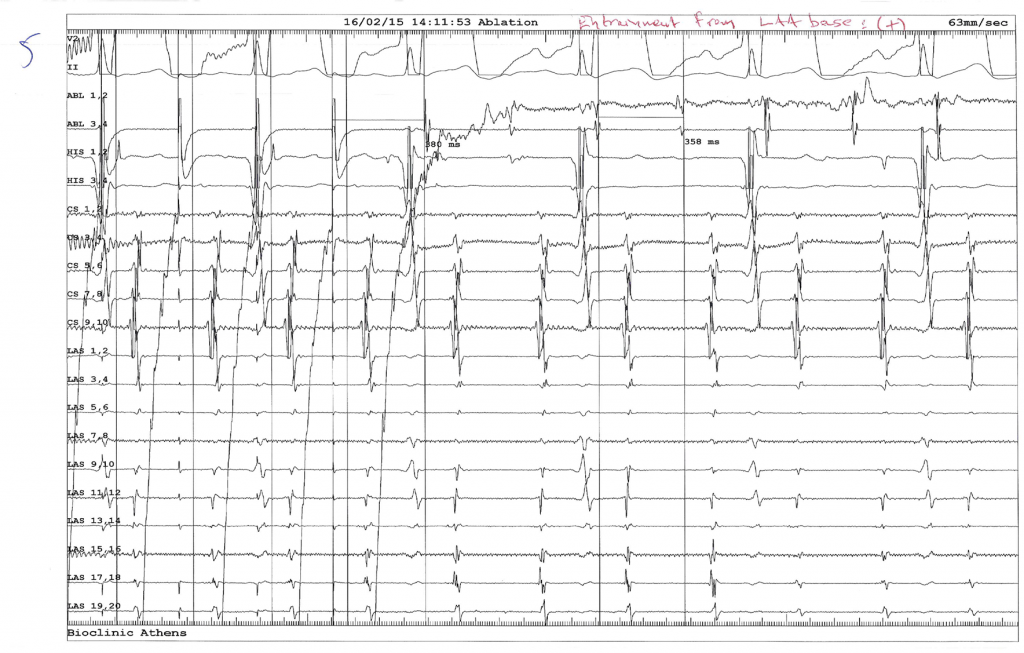
Fig. 5

Fig. 6
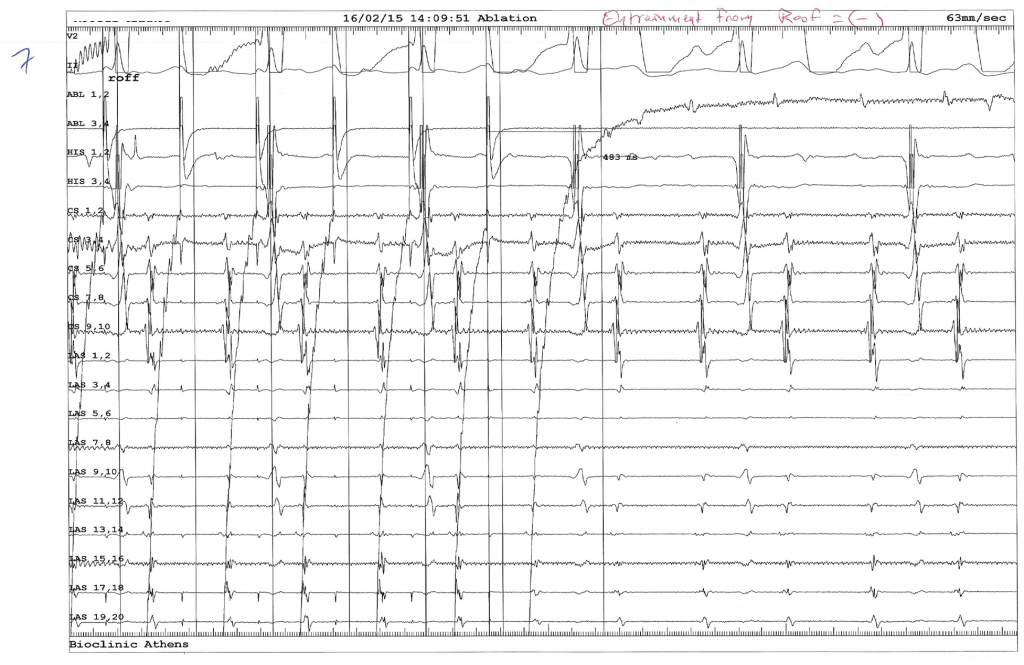
Fig. 7
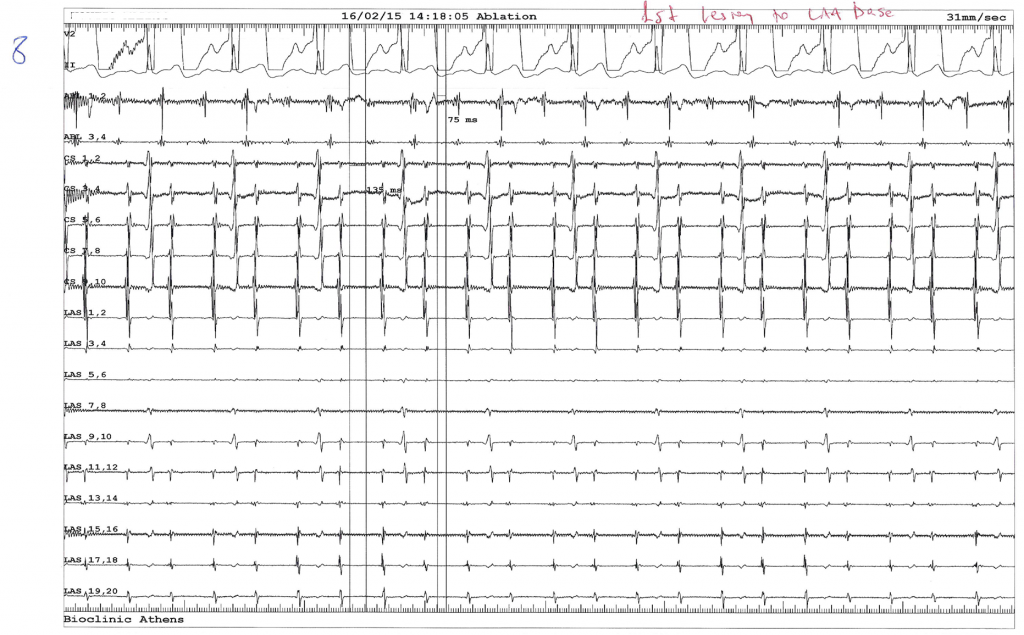
Fig. 8
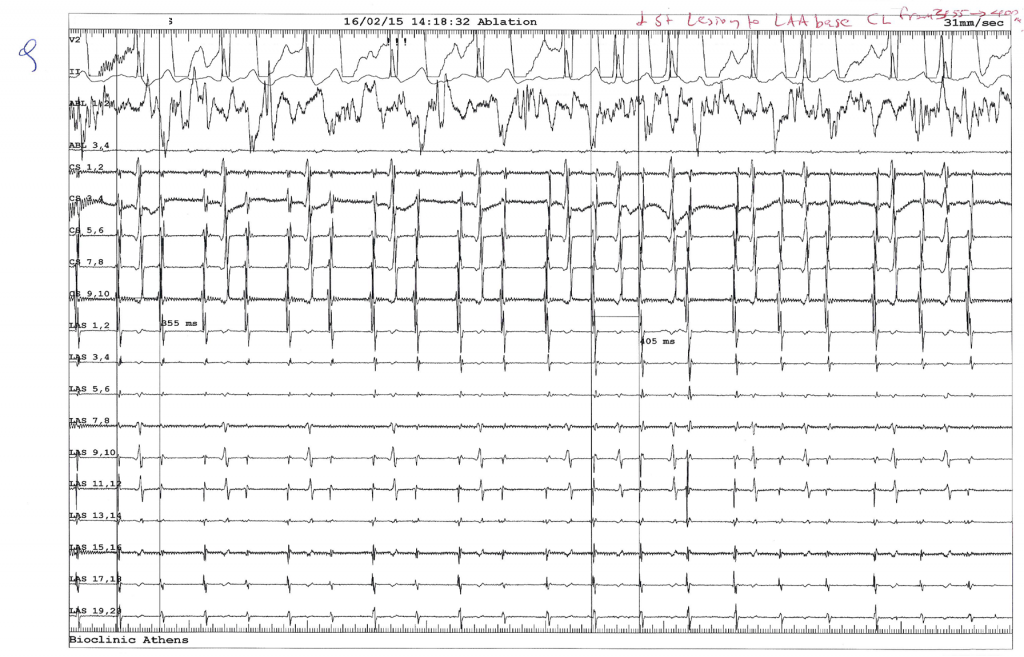
Fig. 9
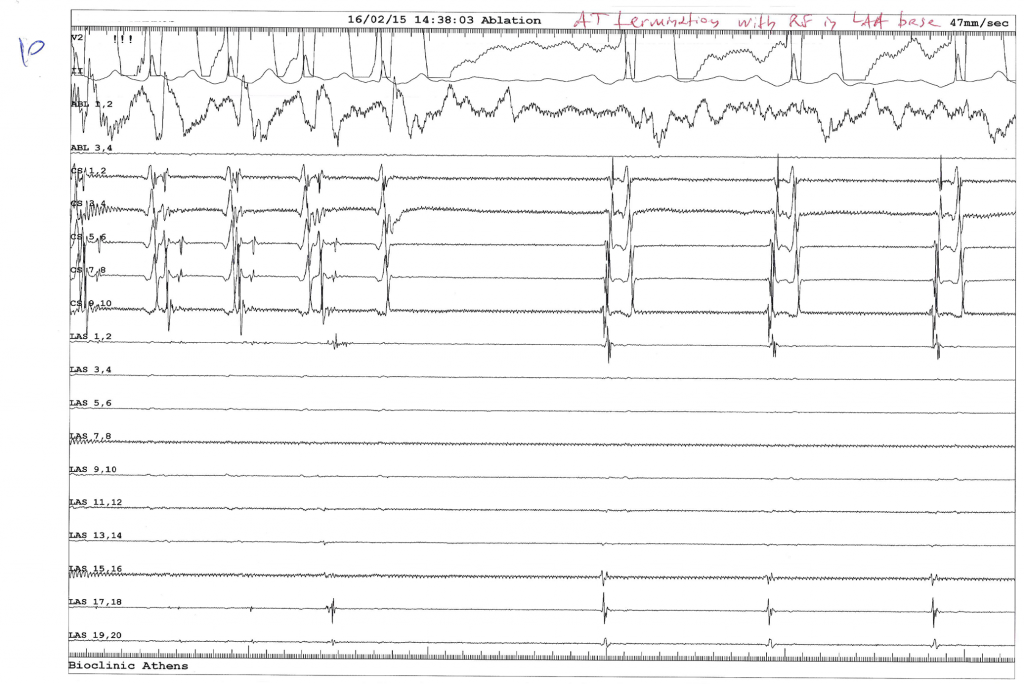
Fig. 10
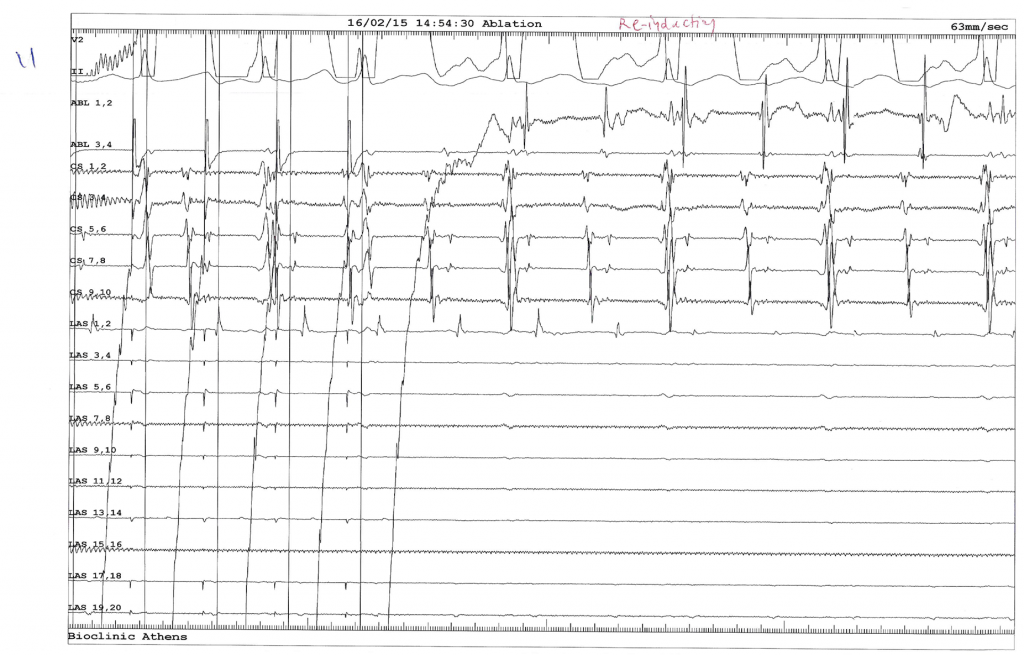
Fig. 11
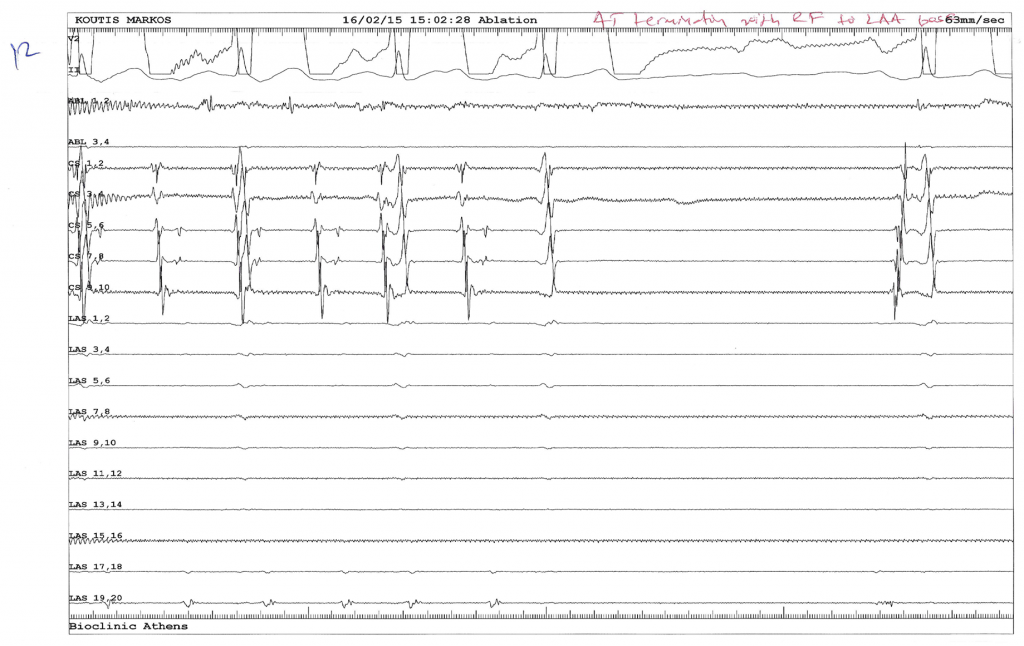
Fig. 12
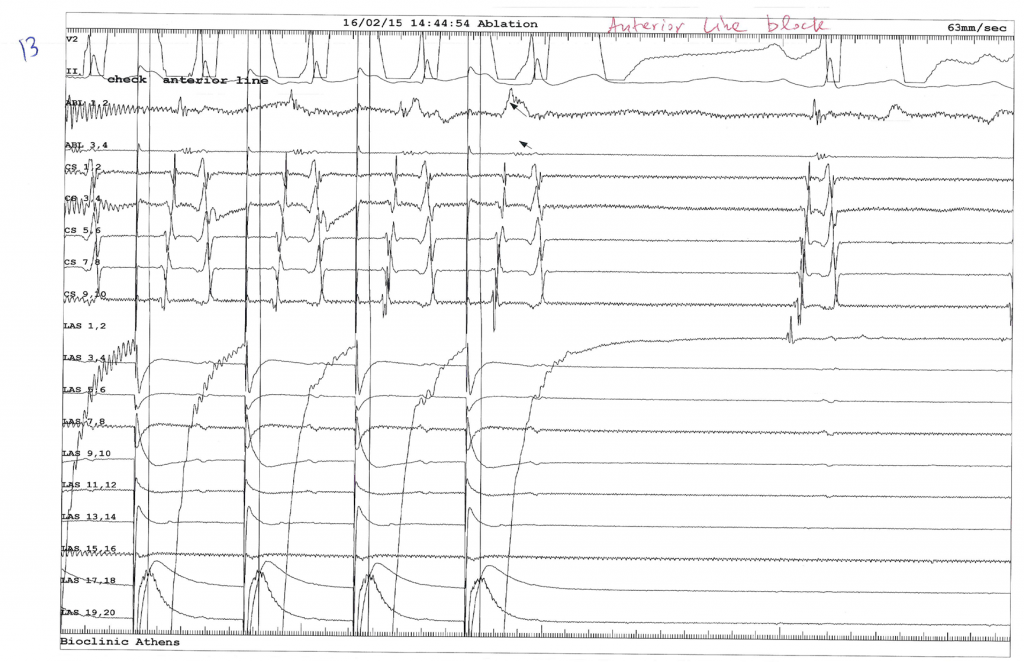
Fig. 13
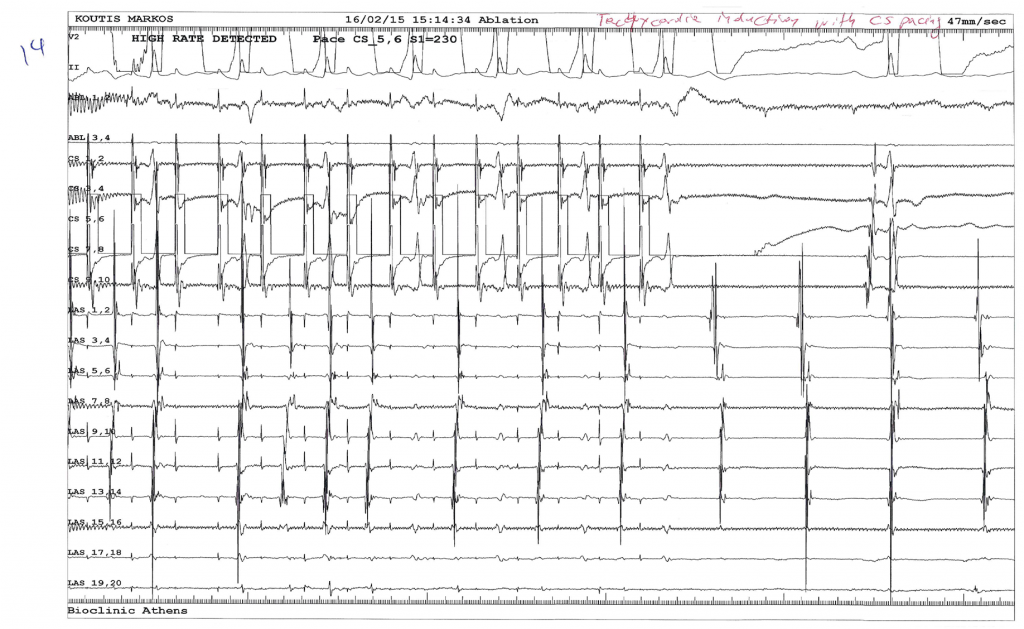
Fig. 14
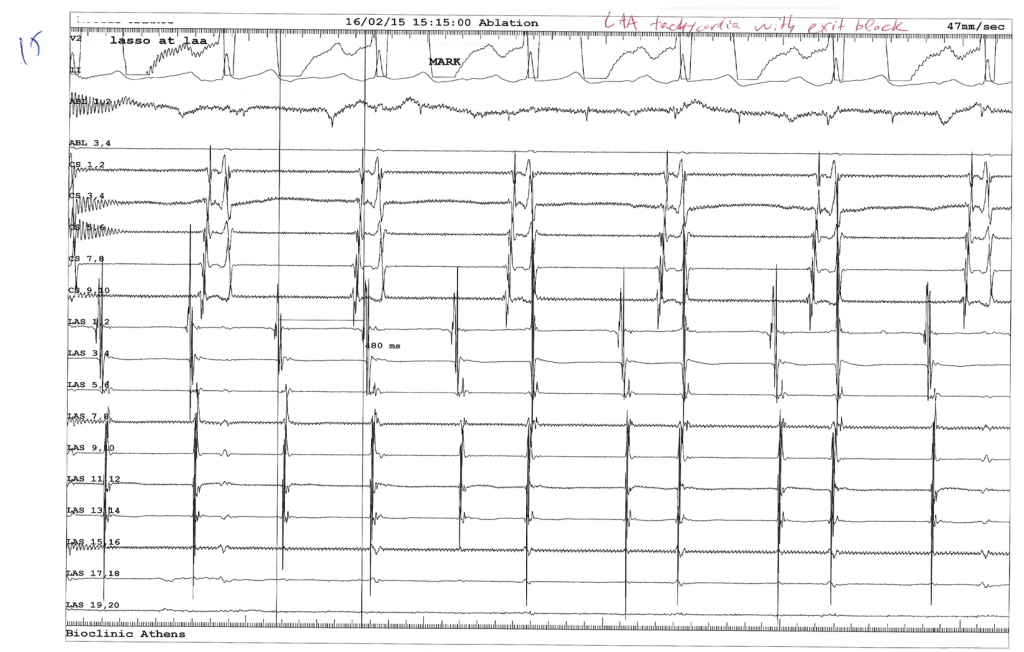
Fig. 15
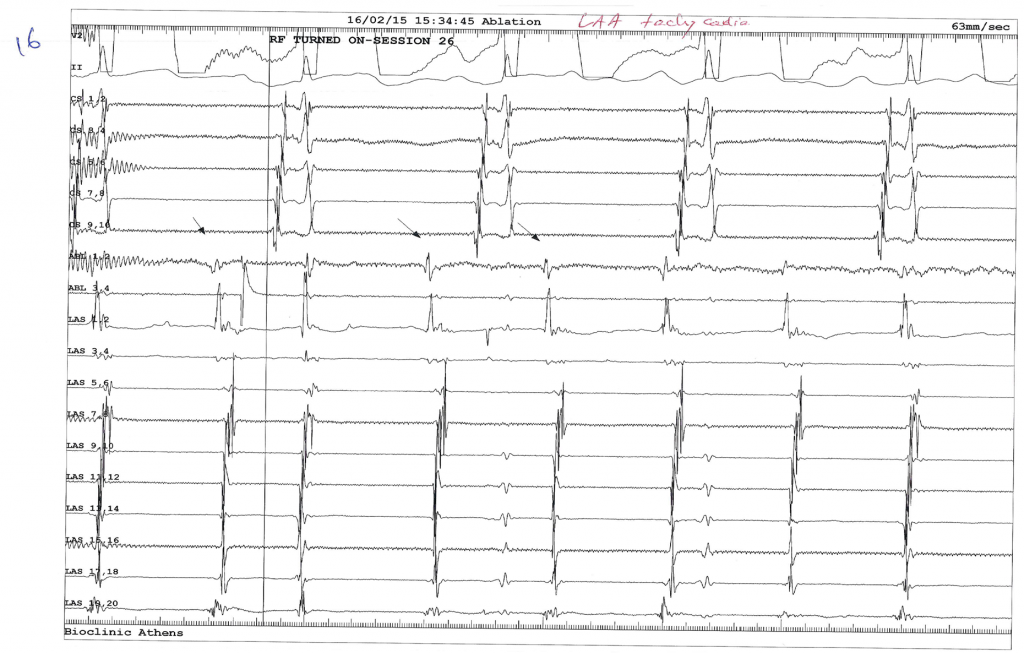
Fig. 16
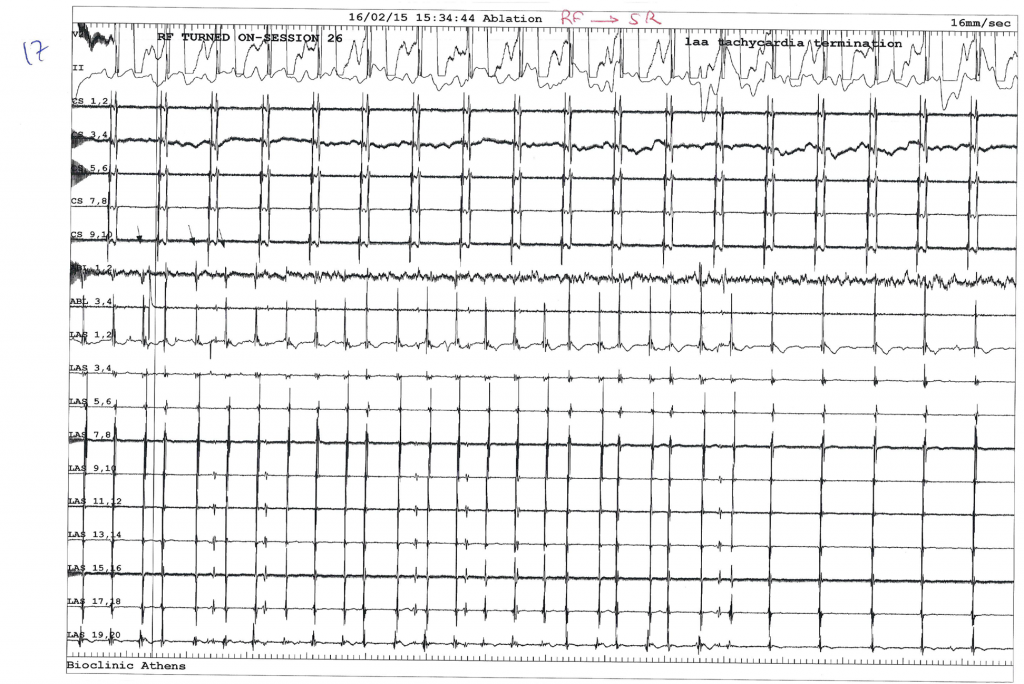
Fig. 17
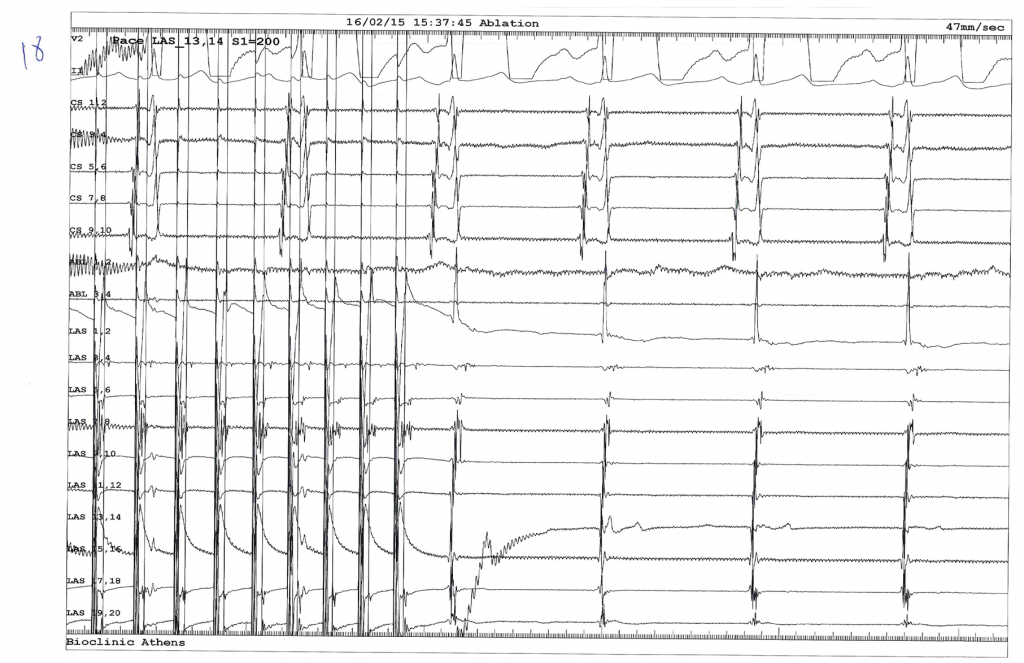
Fig. 18
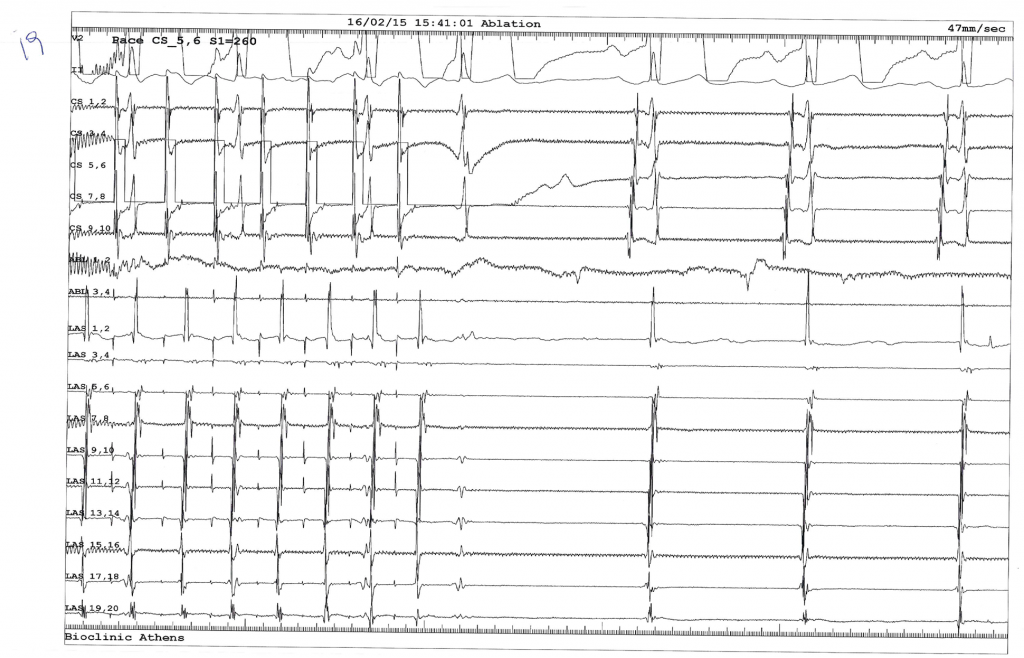
Fig. 19
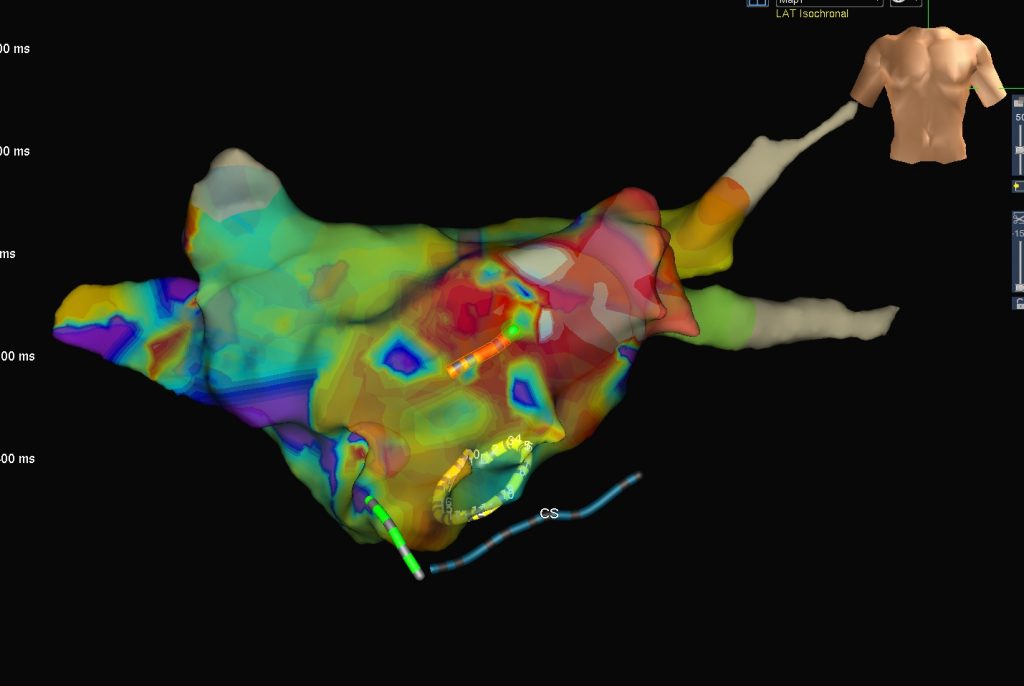
FIG A
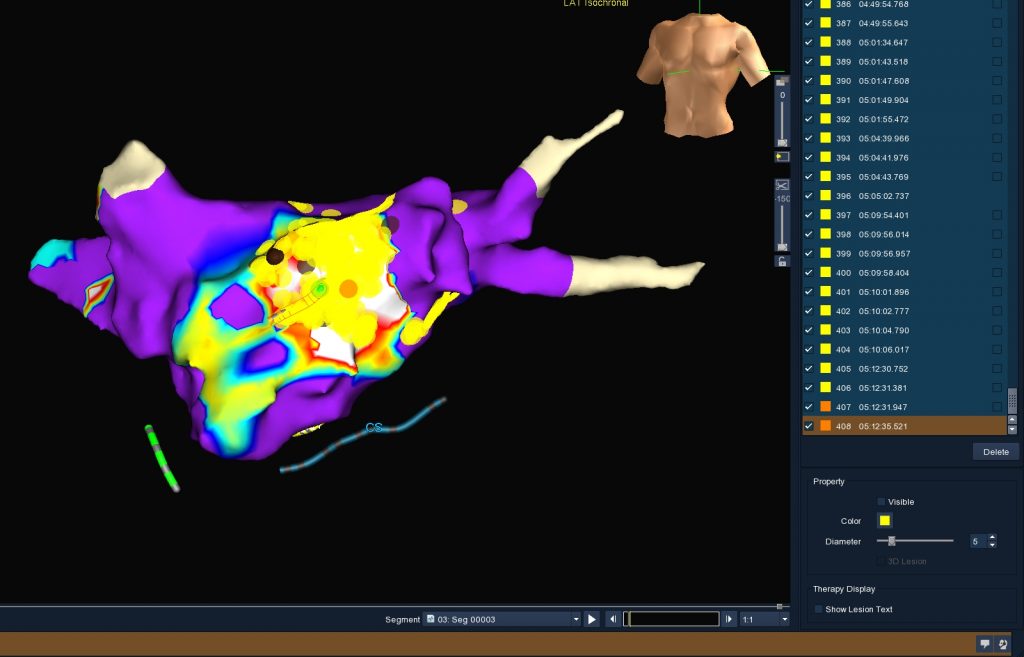
FIG B
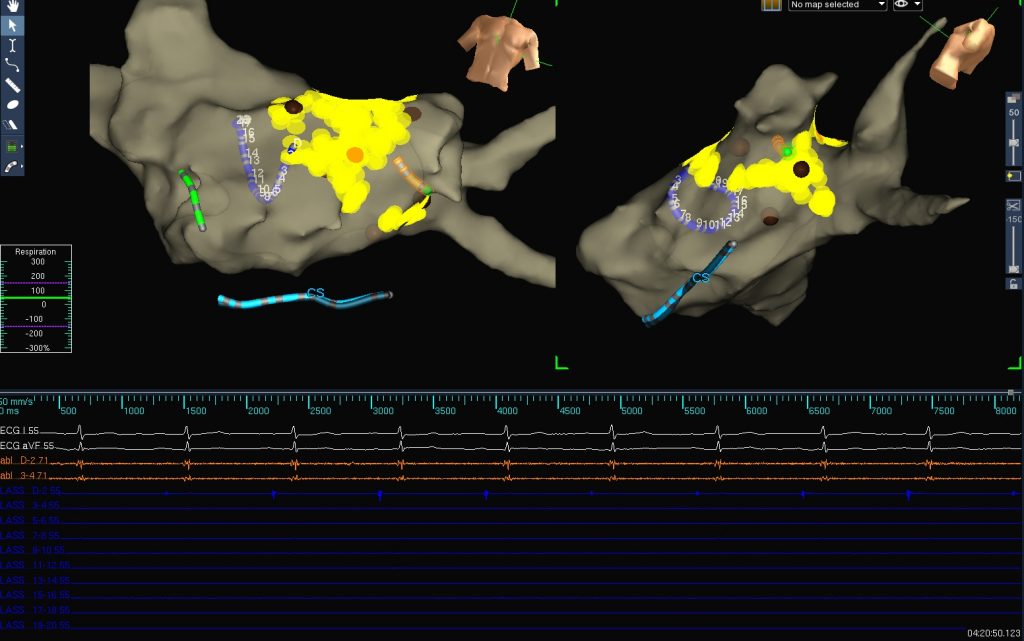
FIG C
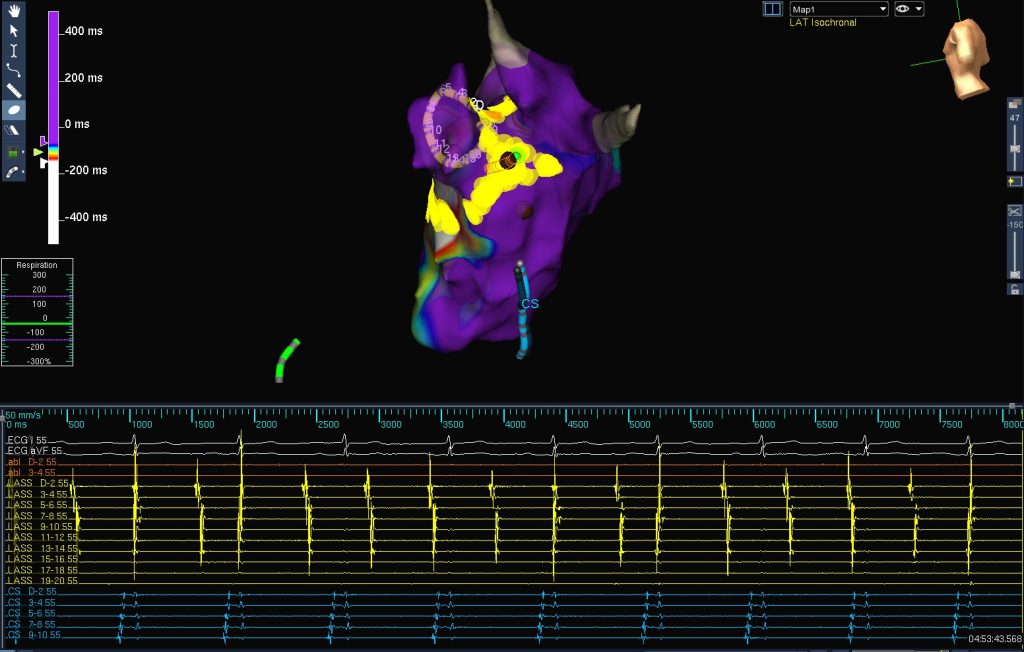
FIG D